Source: https://rwmalonemd.substack.com/p/july-2021-cdc-knew-the-mrna-covid
"They lie to us, we know they're lying, they know we know they're lying, but they keep lying to us, and we keep pretending to believe them"- Solzhenitsyn


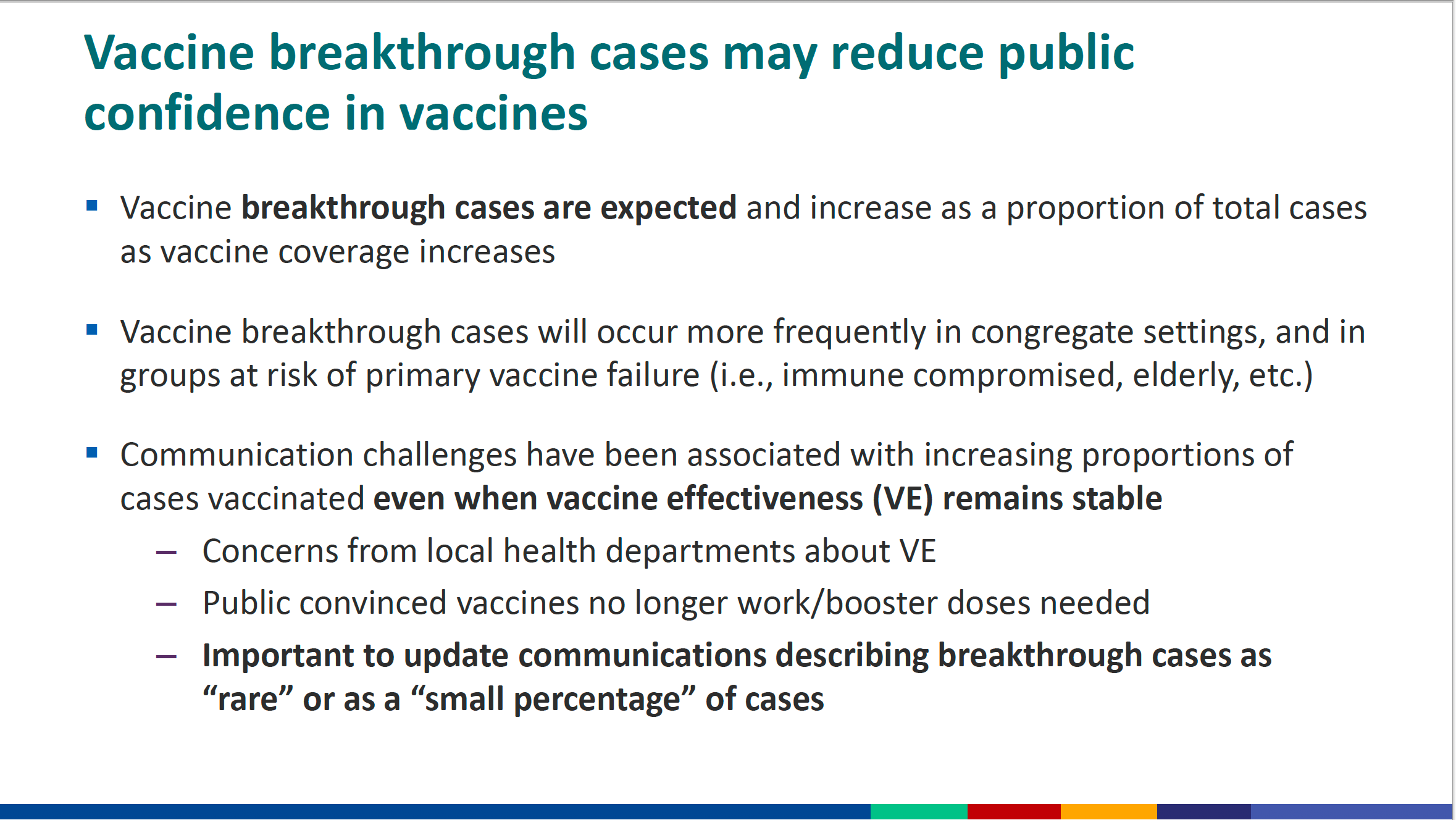
(note: “Improving communications” is a different way of saying “improving propaganda”. “Vaccine Breakthrough” is the CDC’s way of admitting that the EUA authorized “vaccine” products are leaky and not preventing infection, replication, and spread of SARS-CoV-2.)
As the storm clouds of COVID gray and black propaganda coming from our Governments (in close cooperation/partnership with Pharma and academia) continue to pummel all of us, it is useful to revisit the actual timeline and events concerning what the US Government knew and when.
I have previously covered the timeline of the US Government’s awareness of the severity of the myocarditis and pericarditis adverse events associated with all of these US EUA authorized COVID vaccines. That prior reporting built on the excellent work of Zack Steiber of the Epoch Times.
For prior “Who is Robert Malone” substack essays discussing what the US Government knew about Myocarditis and when, see here (Sept 20, 2023), and here (March 08, 2022), and here (Jan 07, 2022).
It is hard to believe that Jill (Dr. Jill Glasspool-Malone) and I have now published over 800 essays on Substack (this is technically #810) going back to the first one, published on November 26, 2021 (154 likes, and only one comment- who could have imagined what would come). What many may not know is that before starting on Substack (at the advice of Steve Kirsh!) I had published many essays with Trial Site News, including this one titled “Bioethics of Experimental COVID Vaccine Deployment under EUA: It’s time we stop and look at what’s going down.“ published May 30, 2021. You can find a bibliography of all of my COVIDcrisis essays published by Trial Site News here.
And of course there were quite literally hundreds of podcasts and interviews, many of which were censored and lost in the sands of time. Also lost to time and censorship were my many comments and essays on LinkedIn. One of the key early podcast interviews was with Dr. Philip McMillan of the UK, recorded live while I was at a horse show (Saturday June 05, 2021). Philip re-posted the interview from within his own Substack on December 17, 2022 in acknowledgment of my repatriation onto what was then known as “Twitter”. Below are a list of topics discussed and associated timecodes. Later today I will record a follow-up podcast with Dr. McMillan revisiting our prior broadcasts (including a September 25, 2021 one with Dr. Geert VanDen Bossche). Stay tuned for that one.
“Truth behind the discovery of mRNA Vaccines” (Drs. Philip McMillan and Robert Malone, June 05, 2021)
Topics and Timecodes:
0:00 Intro
1:45 Who is Dr Robert Malone
4:00 Origin of virus/vaccine technology
9:00 First concept of mRNA vaccines by Dr Malone
15:20 Struggles with PTSD as PhD student in SALK institute
22:40 Feelings of loss over mRNA technology
27:10 Was he surprised at the success of the technology
31:00 Early concerns about potential risks of mRNA vaccine technology
36:10 Why is Dr Malone speaking out about this?
46:40 Views on the biodistribution of mRNA vaccines
50:00 Problems with vaccine bias
53:20 Understanding abnormal signals after vaccines
59:45 Discussing autoimmunity in COVID-19
1:09:27 Is it appropriate for mass vaccination at this point?
1:12:08 Bioethics on covid vaccination in adolescents
Many talk a big talk about having been early in recognizing and discussing the problems with the WHO and USG mismanagement of the COVIDcrisis. But few actually document the actions they took and when they took them. Mine are readily available and quite public. Judge for yourself whether I have been early and accurate in my positions on these issues. I have both talked the talk and walked the walk. Frankly, with this record, I continue to be amazed by the trolls and bots who assert that I am “controlled opposition”. As Bobby Kennedy once stated, “If Robert Malone is controlled opposition, then send me a hundred more like him”.
With that said, below please find an edited version of my Trial Site News publication “The Leaked CDC SARS-CoV-2 Delta Strain Presentation; Key Takeaways” published Aug. 22, 2021. The significance of this essay and associated CDC documentation (released by the Washington Post on July 30, 2021) is that it demonstrates that the US Government was well aware at that time that the Vaccine and Mask mandates were not working, and could not achieve the promised “herd immunity”. Basically, many were forced to accept a leaky and toxic vaccine product that would not prevent infection, replication, transmission, hospitalization or death. So why did the US Government mandate these ineffective public health measures? That is the big question that I hope the special committee currently investigating in the House of Representatives can answer. Because it certainly was not about reasonable public health measures, and certainly did not meet well established transparency and informed consent norms.
(Please keep in mind that this is a historic record of my opinions and evaluations of CDC data circa Aug 22, 2021), and does not reflect my current position and opinion on the matters discussed. The data have evolved since then, and so has my position changed as the data have developed - as should be the case.)
The Leaked CDC SARS-CoV-2 Delta Strain Presentation; Key Takeaways
Robert W Malone, MD, MS
Published Aug. 22, 2021, Trial Site News
https://www.washingtonpost.com/health/2021/07/29/cdc-mask-guidance/
https://www.washingtonpost.com/health/2021/08/18/cdc-data-delay-delta-variant/
July 29, 2021, a confidential internal presentation from the US Centers for Disease Control and Prevention (CDC) inadvertently made its way to the public via the Washington Post. The deck showcased data and thinking concerning the infectivity of the SARS-CoV-2 Delta variant and public health policy that may run against the popular grain. After the Washington Post published a brief article which buried the lede by focusing on CDC communication challenges, the data and implications of the presentation and data have been largely overlooked.
Although we have heard much from the mainstream media about how the Delta SARS-CoV-2 variant is filling up hospitals including pediatric intensive care wards and driving a new wave of preventable deaths, and how we now have a “Pandemic of the Unvaccinated” < https://www.nytimes.com/2021/07/16/health/covid-delta-cdc-walensky.html > driven by misinformation promulgated by a “Dirty Dozen” who spread vaccine “misinformation” < https://www.salon.com/2021/03/30/the-dirty-dozen-a-tiny-group-of-anti-vaxxers-are-flooding-the-internet-with-misinformation/ >, information leaked to the Washington Post has revealed that much of the truth about Delta has been hidden or otherwise misrepresented to the public by the CDC. What was leaked runs contrary to the dominant narrative pushed by the Biden administration and the press. This leaked information was superficially covered and then quickly vanished from public awareness. In terms of the general public, perhaps this is for the best- why focus on inconvenient truths when there is so little that the public can do to mitigate the impact on their daily lives? However, TrialSite is not designed to provide information to a general audience, but rather to those involved in medical product development and the clinical research community. Analysis of inconvenient COVID-19 medical truths are important for our readership, because they impact on clinical trial design, data analysis, decision making, and all strategic and tactical aspects of medical product development planning.
In support of our unique readership, TrialSite is providing a brief overview and analysis of key slides in the leaked presentation. The goal is to help identify internal information which the CDC has sought to avoid disclosing to the general public, but which is critical for our readers and the industry in which they work. To follow along, please see the power point presentation available at https://www.nih.gov/news-events/news-releases/nih-begins-study-covid-19-vaccination-during-pregnancy-postpartum
In side #2 of the presentation, the recommended public health messaging challenges and recommendations for wording to be used when communicating with the press and public are highlighted. Review of the following slides #3 to #5 illustrates the CDC focus on COVID-19 clinical outcomes rather than breakthrough infection and transmissibility, and indicates an inflection point in April 2021 beyond which both hospitalization and death endpoints for vaccinated begun to climb. Of interest in slide #4 is the slope of the rise in deaths in the vaccinated is greater than that of the rise in hospitalization. A similar paradox is also seen in the more recent UK datasets concerning Delta infections in vaccinated individuals, and this has been a persistent finding in those data. This trend should be closely monitored, and if persistent and statistically significant, raises concerns that this may indicate signs of antibody dependent enhancement. Given the recent information concerning poor durability of the genetic vaccines (Moderna, Pfizer, J&J), subanalysis of these data based on time post completion of vaccination would be useful (eg, <6 months post, >= 6 months post vax). Such an approach might help clarify the contribution of waning immunity to this effect.
Slides #6 through #13 focus on currently available vaccine effectiveness (VE) data. VE calculations provided primarily focus on death and disease, show reduced effectiveness compared to earlier projections, and predominantly cover a blended time frame in which contributions from Beta predominates and Delta infection is minimal or non-existent. In contrast, recent reports from Israel (from Delta) indicate Pfizer vaccine effectiveness of less than 40% in preventing breakthrough infections.
The CDC information, analyses and interpretations concerning the Delta variant of SARS-CoV-2 are included in slides #14 through #22. These include a number of surprising findings as well as some rather odd internal contradictions. Slide #15 is pivotal and establishes broad context for how CDC assesses the public health threat posed by Delta. From this slide we learn that the CDC believes that Delta infection poses approximately the same risk for death from disease as posed by the original ancestral strain, but is as infectious as “chicken pox” (varicella-zoster virus), which has a baseline reproductive coefficient (Ro) of approximately 8- about 2.5 times the Ro of the ancestral strain. Furthermore, as summarized in slides #16 and 17, the viral load observed during Delta infection (breakthrough or primary infection) is significantly higher than observed with the ancestral strain. Delta titers are at least as high in previously vaccinated as in unvaccinated. Slide #19 summarizes data then available concerning reduced vaccine effectiveness for the Delta strain relative to the ancestral Alpha strain, although more recent data from Israel indicate that Pfizer vaccine effectiveness against Delta infection is under 40%.
Among the most surprising and alarming aspects of the entire presentation are the epidemiologic risk management modeling findings presented Slides #20 and #21.
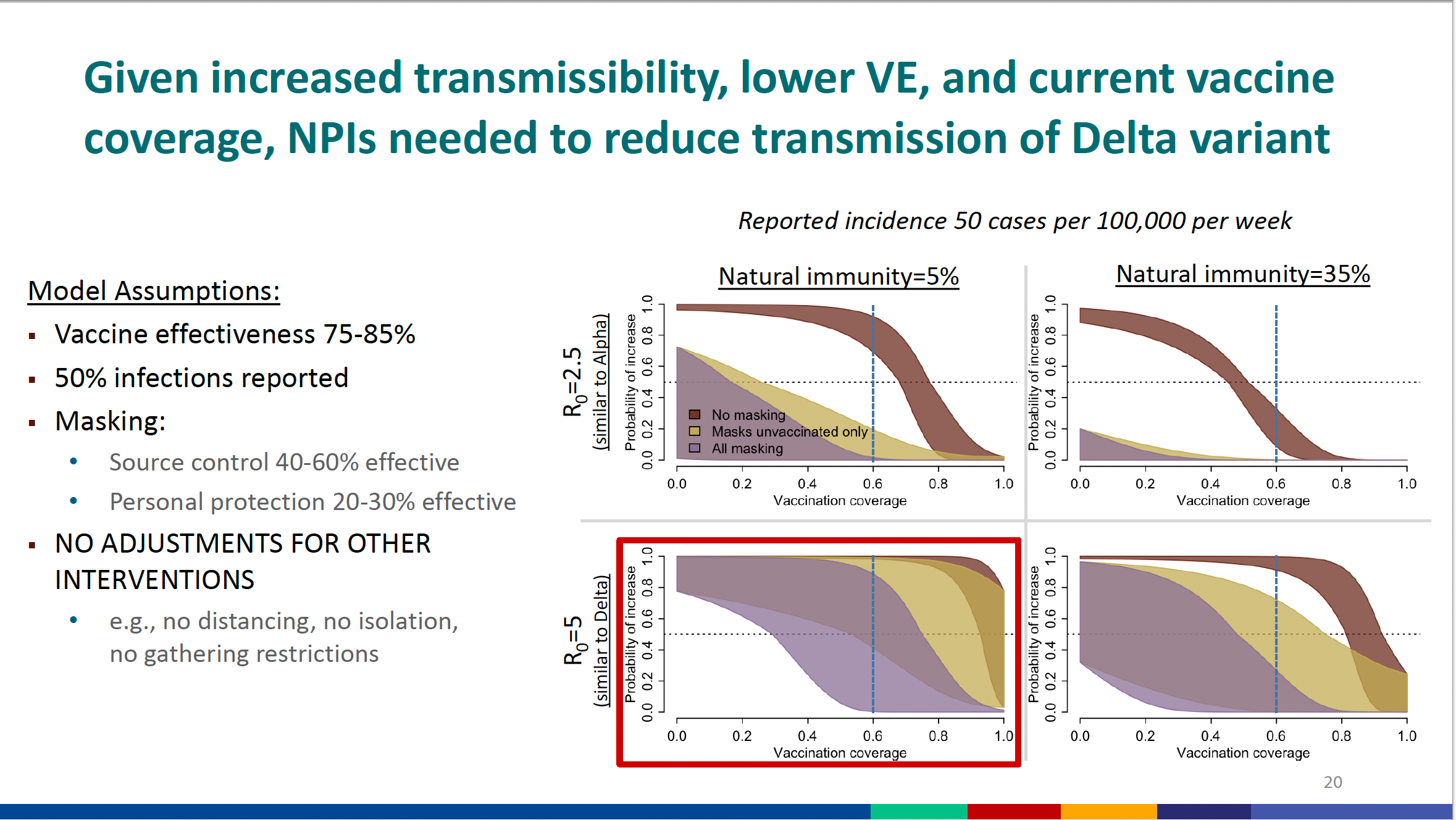

This pair of slides are complicated and difficult to understand for those who have not previously encountered these types of analyses, which may explain why the Washington Post did not discuss the information and conclusions. These represent statistical modeling projections for the potential impact of different intervention options (vaccination and mask use) based on assumptions concerning the reproductive coefficient of the virus, the effectiveness of mask or vaccine use, the extent of vaccine acceptance in the population (uptake), and the fraction of the population which has been previously exposed/recovered/naturally immune due to prior SARS-CoV-2 infection. The NPIs mentioned in the title refers to non-pharmaceutical interventions (ergo masks, social distancing, etc.). The starting point for understanding these projections is to understand the underlying assumptions of the modeling performed; 1) Vaccination is presumed to 75-80% effective in preventing infection (but the most recent data indicate that approximately half that value is a more reasonable assumption). This is a measure of the “leakiness” of the vaccines, which here is assumed to be 20-25%, but is more likely to be about 60%. 2) The Ro is presumed to be 5 for these models (Ro = 2.5 for Alpha), but in Slide #15 we learned that the Delta Ro is 8. 3) “Natural Immunity” from prior infection/recovery is presumed to be either 5 or 35% of the population. 4) The baseline “incidence” of new cases of infection is presumed to be 50 cases/100,000 population/week. 5) The benefits of mask use in preventing infection of those wearing a mask is presumed to be 20-30%, whereas the benefits for blocking virus transmission from infected persons is presumed to be 40-60% effective. The vertical axis projects the probability that the 50 new cases/100,000/week increases based on the modeled interventions (vaccine uptake, mask use). The horizontal axis projects the fraction of the overall population which has been fully vaccinated (eg. 0.6 = 60% vaccine uptake). Based on the “red box” designation, CDC appears to presume that 5% of the overall population currently has “natural protection” from prior infection and recovery. The darker brown curve represents the probability range of viral spread (increase) if no mask use (vaccine intervention alone). The mustard-colored curve reflects the modeled effect of just masking the unvaccinated. The purple curve indicates the modeled effect of masking on both vaccinated and unvaccinated. These mask effectiveness ranges are the reason why the curve plots are so broad, rather than just being a single line. Based on the flawed assumptions used (those flaws being that Ro is actually 8, not 5, and vaccine effectiveness is more like 40%), these projections indicate that at approximately 60% vaccine uptake (also a bit optimistic at this point), in the absence of mask use the Delta variant has an approximately 100% probability of spreading at greater than 50 cases/100,000/week. If only the unvaccinated were to wear masks, the probability of seeing further spread ranges from 40 to 100%. If both vaccinated and unvaccinated practice optimal mask use, the probability of further Delta viral spread ranges from 0 to 90%. From this analysis (Slide # 22), the CDC concludes that “Given higher transmissibility and current vaccine coverage, universal masking is essential to reduce transmission of the Delta variant” (below 50 cases/100,000/week). Based on these projections, it appears that if the more realistic variables of Ro =8, 40% vaccine effectiveness, and suboptimal mask use are employed, it is unlikely that the eventual spread of the Delta variant through the general population can be controlled even with considerably higher uptake of these leaky vaccines and perfect mask compliance.
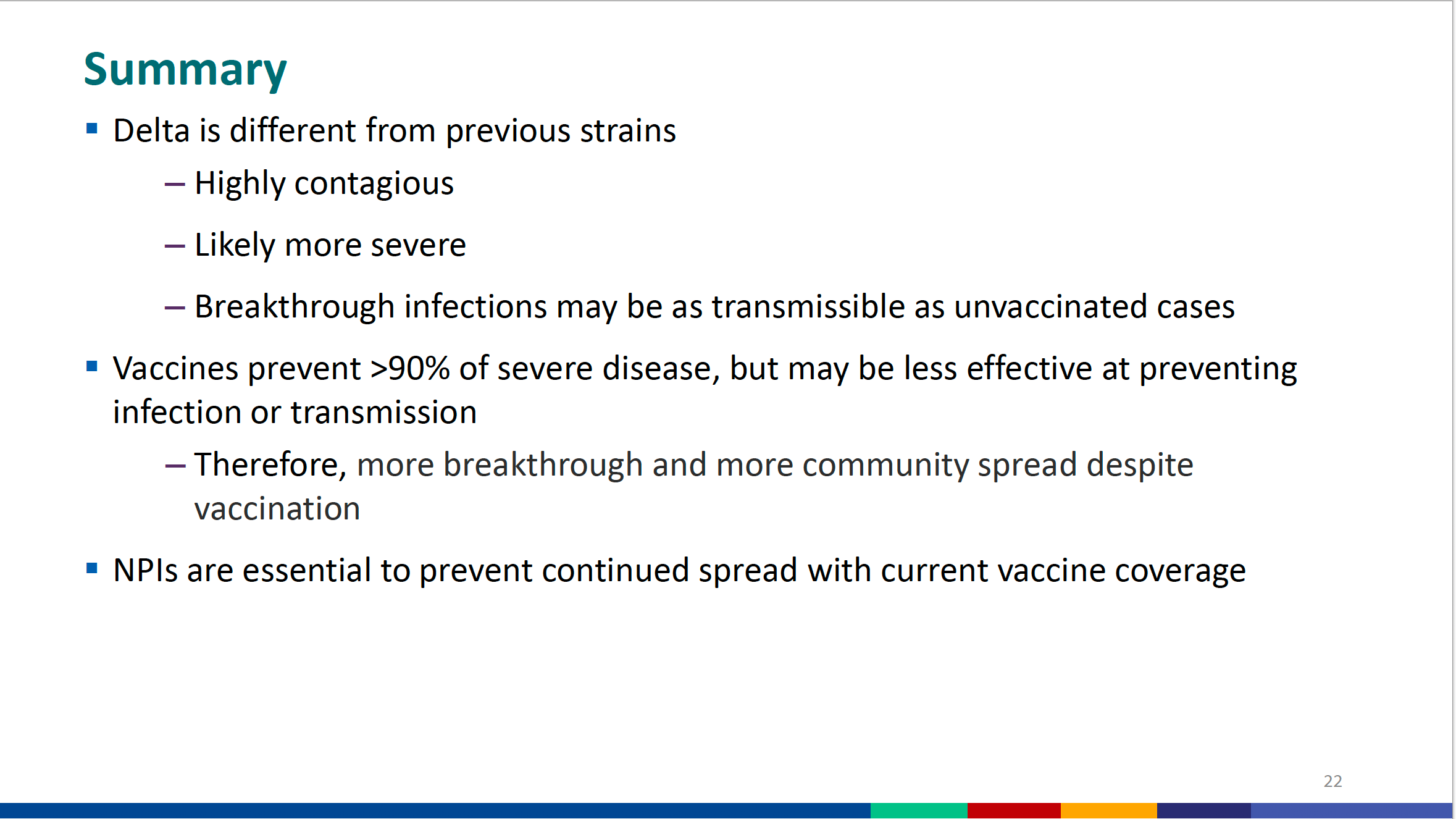
Slide #22 pretty much sums up the bleak situation. Called “Summary” the CDC summarizes the following; 1) Delta is highly contagious and likely more severe (the latter point is contradicted by slide #15 as well as more recent data). 2) “Breakthrough” infection cases are just as likely to infect others as infections of those not previously vaccinated. 3) Vaccination appears to still prevent more severe disease from Delta compared to those who are unvaccinated (however both slide #4 and UK data show a paradoxical increase in death in vaccine breakthrough cases relative to severe disease). 4) Vaccination alone cannot stop the spread of Delta. Non-pharmaceutical interventions (mask use) will also be needed (but the data indicate that even full mask compliance will only slow the spread).
How to Transcend this Crisis?
Of course the answer would depend on one’s point of view. The following actions should be considered:
· Provide personal risk assessment tools
Provide clear and complete data on vaccination risks
· Offer vaccination to high risk individuals
· COVID is complex, with different stages. Allow physicians to practice evidence -based medicine guided by laboratory tests
· Use sequence-independent, stage appropriate medicines (Ivermectin, Famotidine/Celecoxib, Fluvoxamine, Apixaban, Vitamin D, etc.). Aggressive and early treatment is critical.
Emphasize treating patients as soon as they develop the disease (outpatient)
· Stop censoring and blocking repurposed drug development
· Think precision evidence-based medicine guided by laboratory test values
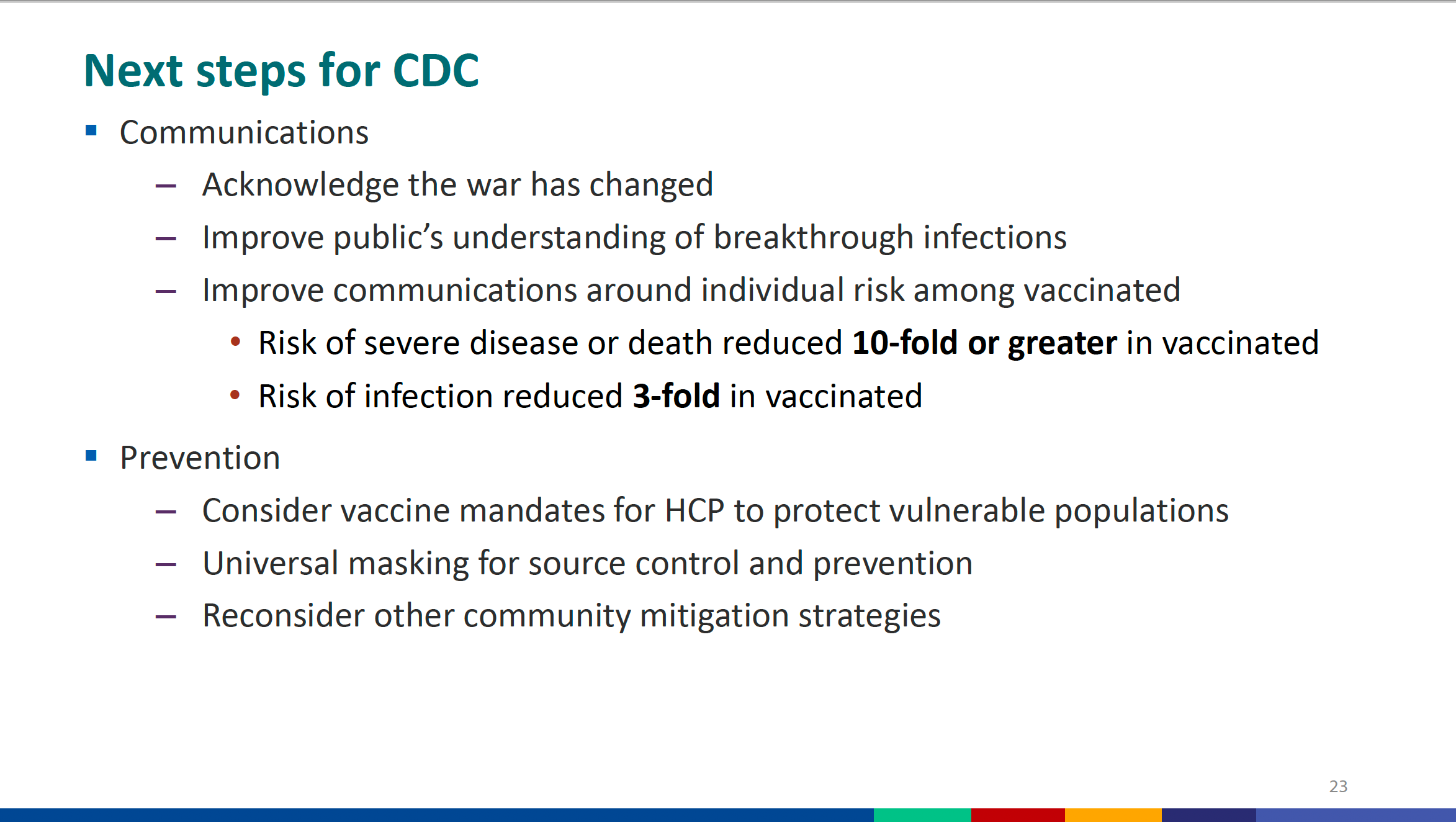
Finally, in contrast to the message and information management strategy which CDC proposes in slide #23, the following messaging strategy is proposed;
· Public health campaigns should be positive, ethical, truthful & empathic.
· People should feel empowered when making health choices.
· In both actions and words It's important to steer clear of fear, coercion and questionable ethics...for the present, but arguably mostly for the future.
· Obey federal law concerning bioethics (common rule) and be transparent about risks as well as benefits. Do not circumvent time tested processes and ethics.
· Trust, educate, and respect citizens right to choose
· Public health messaging should avoid authoritarian demands, information censorship, and psychological manipulation via big media and big tech.
No comments:
Post a Comment
Note: only a member of this blog may post a comment.